For years, the prevention of cardiovascular disease (CVD) has centered on a single metric: LDL cholesterol. The prevailing belief was simple—reduce LDL and heart disease risk would naturally decline. But despite routine cholesterol testing and increasingly aggressive LDL-lowering therapies, cardiovascular disease remains the world’s leading cause of death.
The scale of the problem is staggering. Cardiovascular diseases account for more than 17 million deaths each year, with annual fatalities expected to approach 24 million by 2030¹. These trends are not isolated, they are interconnected and largely driven by a shared underlying issue: metabolic dysfunction.
This raises a difficult but unavoidable question—have we been prioritizing the wrong indicators when it comes to predicting heart disease?
The LDL Paradox
LDL cholesterol plays a role in atherosclerosis, but on its own it is a weak predictor of cardiovascular events2. Large studies have found that many people who develop heart disease don’t have high LDL-C, highlighting the limits of using LDL alone to assess risk3.
It underscores that LDL alone fails to capture the complex underlying biology of cardiovascular disease.
The Real Driver: Metabolic Dysfunction
Cardiovascular disease is increasingly understood as a downstream consequence of insulin resistance and impaired energy metabolism. Insulin resistance triggers a cascade of changes that directly accelerate atherosclerosis, including elevated triglycerides, reduced HDL cholesterol, an increase in small, dense LDL particles, chronic inflammation, endothelial dysfunction, and a heightened tendency toward clot formation4.
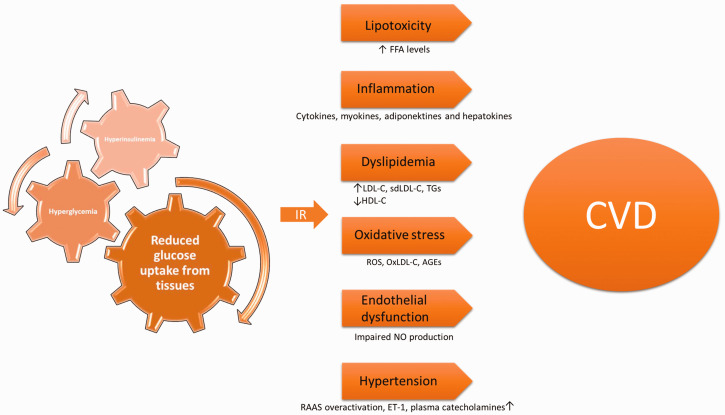
Collectively, these abnormalities define metabolic syndrome, a condition that significantly elevates cardiovascular risk, even when LDL cholesterol appears “normal.”
Long-term research comparing dozens of biomarkers shows that markers of insulin resistance predict premature heart disease up to six times more strongly than LDL cholesterol. Even advanced lipid markers such as Apolipoprotein B (ApoB) provide valuable insight, but in many cases, metabolic indicators offer additional context that may enhance cardiovascular risk assessment.
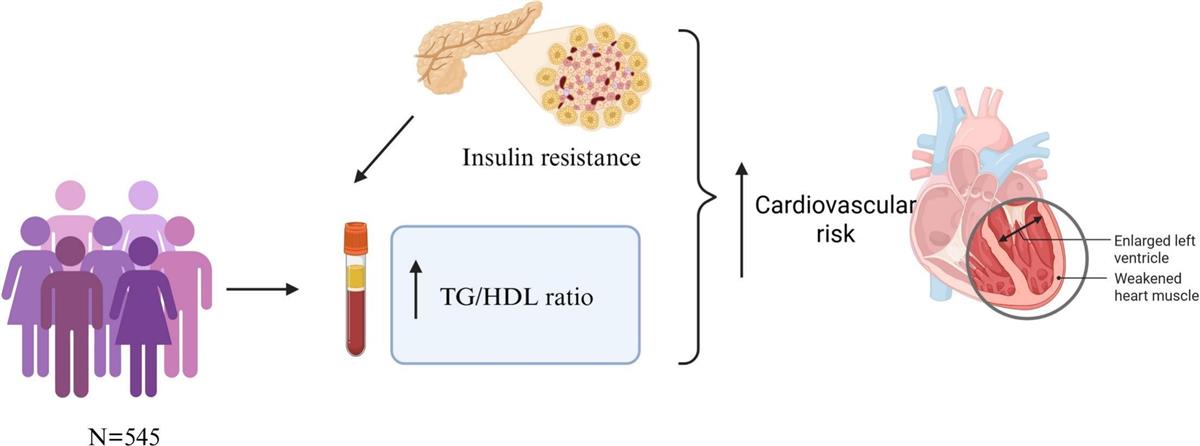
The Triglyceride-to-HDL Ratio: A Practical Tool5
Among metabolic markers, the triglyceride-to-HDL (TG/HDL) ratio stands out for its simplicity and clinical relevance. Derived from a standard lipid panel, it serves as a reliable proxy for insulin resistance and small, dense LDL particles, both strongly linked to cardiovascular events.
General interpretation (mg/dL):
- < 2 → favorable metabolic health
- 2–3 → emerging insulin resistance
- > 3 → high cardiometabolic risk
Across multiple studies, higher TG/HDL ratios are associated with significantly increased rates of heart attack6 and cardiovascular death, even when LDL levels are identical. In comparative analyses, TG/HDL consistently outperforms LDL in predicting outcomes, reinforcing a key insight: metabolic context matters more than cholesterol concentration alone.
Insulin Resistance: The Common Thread
The International Diabetes Federation estimates that 537 million people were living with diabetes in 2021, a figure projected to rise to 642 million by 2040. Insulin resistance is closely linked to obesity, type 2 diabetes, non-alcoholic fatty liver disease, hypertension, PCOS, and heart failure. Its relationship with heart failure is particularly concerning—insulin resistance increases heart failure risk, while heart failure further worsens insulin sensitivity, creating a self-perpetuating cycle.
South Asian (SA) individuals are at increased risk for developing diabetes and cardiovascular disease (CVD) at lower body mass index (BMI), as compared to other racial/ethnic groups. While cardiovascular disease is the leading cause of death globally, South Asian individuals (from India, Sri Lanka, Pakistan, Bangladesh, Nepal, Maldives, and Bhutan) represent 25% of the world’s population and have the largest proportion of individuals affected by cardiovascular disease7.
A Comprehensive Approach to Cardiovascular Risk Assessment
A more comprehensive assessment of cardiovascular risk goes beyond conventional lipid parameters by linking metabolic markers to measurable tests. Indicators such as the TG/HDL ratio and insulin resistance can be effectively evaluated through laboratory tests including fasting insulin, HbA1c, Apolipoprotein B (ApoB), hs-CRP, and IL-6, providing deeper insight into underlying metabolic and inflammatory processes.
Suggested Screening Approach: Begin with a standard lipid panel and calculate the TG/HDL ratio to identify early metabolic imbalance. This should be complemented with HbA1c and fasting insulin to assess glycaemic control and insulin resistance. In patients with higher or unclear risk, adding ApoB and hs-CRP can further refine cardiovascular risk stratification, enabling a more targeted and proactive approach to prevention.
A Shift in Cardiovascular Prevention
The evidence is clear: cardiovascular risk is driven more by metabolic health than by LDL cholesterol alone. Effective prevention must move beyond LDL-centric targets and prioritize insulin sensitivity, triglycerides and HDL ratio, glucose regulation, visceral fat, and lifestyle factors such as sleep, physical activity, and nutrition.
LDL cholesterol is not irrelevant, it explains part of the risk, but metabolic dysfunction determines how the risk manifests. Metrics like the TG/HDL ratio offer a more accurate and actionable view of true cardiovascular risk. Reducing the burden of heart disease will require a shift in focus, from chasing cholesterol numbers to restoring metabolic health at its foundation.
References:
- Hong Sun, Pouya Saeedi, Suvi Karuranga, et al., IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045, Diabetes Research and Clinical Practice, Volume 183, 2022, 109119, ISSN 0168-8227, https://doi.org/10.1016/j.diabres.2021.109119.
- Kendrick M. Assessing cardiovascular disease: looking beyond cholesterol. Curr Opin Endocrinol Diabetes Obes. 2022;29(5):427-433. doi:10.1097/MED.0000000000000761
- https://www.uclahealth.org/news/release/most-heart-attack-patients-cholesterol-levels-did-not-indicate-cardiac-risk
- Kosmas CE, Bousvarou MD, Kostara CE, Papakonstantinou EJ, Salamou E, Guzman E. Insulin resistance and cardiovascular disease. J Int Med Res. 2023;51(3):3000605231164548. doi:10.1177/03000605231164548
- Velia Cassano, Graziella D’Arrigo, Mercedes Gori, Giovanni Tripepi, et al., Possible correlation between Triglyceride/HDL ratio and subclinical myocardial damage in patients with cardiovascular risk factors,
- da Luz PL, Favarato D, Faria-Neto JR Jr, Lemos P, Chagas AC. High ratio of triglycerides to HDL-cholesterol predicts extensive coronary disease. Clinics (Sao Paulo). 2008;63(4):427-432. doi:10.1590/s1807-59322008000400003
- Wolf RM, Nagpal M, Magge SN. Diabetes and cardiometabolic risk in South Asian youth: A review. Pediatr Diabetes. 2021;22(1):52-66. doi:10.1111/pedi.13078